0 Comments
tapping the central glenoid hole for a screw without a guide may enlarge the hole. Using a guide makes the tap inline with the drill hole; this may be better when using a wedge augment
.A PSI guide helps execute the preoperative plan.
If the surgeon choses to check the position of the guide using the floor as a reference to check inclination, an error may occur because of the positioning of the scapula. This may happen if an assist arm is used Which is the best option for glenoid baseplate fixation in the elderly? Here are some variables to consider: 1. A 6.5 mm screw is often used. Will this gain sufficient purchase in the elderly?
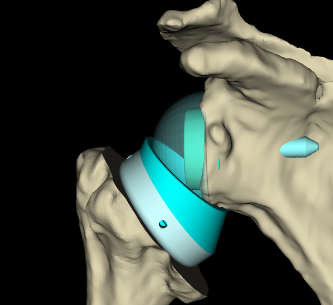
2. A central post has the potential of ingrowth but has a larger diameter of a 6.5 mm screw. 3. A revision of a post will need at least a 9.5 mm screw or a completely different hole position 4. The dimensions of the glenoid vault will determine post perforation which may not be desirable The inlay stem offers specific advantages
1. bone conservation 2, easier revision 3. less calcar resorption 4. helpful in small patients 5. less tendency to stuff the joint IMO, importing the post operative xray image into the software program may be helpful. assessment of lateralization, distalization, DSA and positioning of the implant
a DSA between 40° and 65° results in better active anterior elevation and abduction
 using an inlay system, the DSA is reduced to 62 degrees and distatlization is 17 mm  Maybe distalization greater than 20-25 mm may result in a difficult reduction. A lower neck cut, smaller sphere , or using an inlay stem are options. I think (opinion) the preop planning software to include DSA to anticipate tightness of shoulder reduction
The COR was medially displaced by 28 4 mm with the Delta prosthesis and by 19 3 mm with the Encore prosthesis Matthew D. Saltzman, MDa , Deana M. Mercer, MDc , Winston J. Warme, MDb , Alexander L. Bertelsen, PA-Cb , Frederick A. Matsen III, MDb, *  : Frederick A. Matsen III, MD, Department of Orthopedics and Sports Medicine, University of Washington Medical Center, Box 356500, 1959 NE Pacific St, Seattle, WA 98195. E-mail address: [email protected] (F.A. Matsen III). 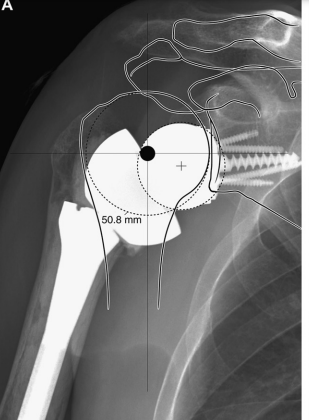  Causes of a tight shoulder with a reverse shoulder arthroplasty: SUPERIOR HUMERAL MIGRATION MEDIALIZED HUMERUS TIGHT CAPSULE HIGH NECK CUT EXCESSIVE LATERALIZATION OF BASE PLATE EXCESSIVE LATERALIZATION OF SPHERE LARGE MUSCULAR MALE LOW GLENOSPHERE OVERSIZED GLENOSPHERE ONLAY SYSTEM INTACT ROTATOR CUFF PRIOR SURGERY PREOPERATIVE STIFFNESS LARGE DELTOID INCOMPLETE PARALYSIS FAILED INTERSCALENE BLOCK Expect a tight reduction of the reverse shoulder if the preop planning software shows a distalization greater than 20 mm and DSA angle greater than 60 degrees in my opinion. This is not validated.
|
CommunityShare your insights and experience with total and reverse shoulder replacement surgery; please reference link to www.completeshoulder.com CategoriesArchives
December 2022
Categories |



 RSS Feed
RSS Feed